
Fibrous Dysplasia
Description of Fibrous Dysplasia
- Fibrous Dysplasia is a benign, slowly progressive disease of the bone, and usually presents in children and young adolescents. In this disease, normal cancellous bone is replaced by fibrous tissue and immature woven bone. It was initially described by von Recklinghausen in 1891, and given the name ‘fibrous dysplasia’ by Lichtenstein in 1938. The etiology of fibrous dysplasia is usually unknown.
- There are three forms of the disease: 70% cases are ‘monostotic’ involving only one bone or contiguous bones, while 30% of cases are ‘polyostotic’ involving several distinct areas of the skeleton, and Polyostotic fibrous dysplasia as a part of McCune Albright Syndrome, accompanied by skin pigmentation and endocrine disorders constituting 3% of polyostotic cases.




Symptoms and Signs of Fibrous Dysplasia
- Fibrous dysplasia most often presents with pain, swelling and disfigurement due to fibroblastic expansion of the involved parts. They also present with visual impairment, bulging of the eyeball, craniofacial swelling, headaches, periorbital pain, and epiphora.
- The most common neurologic complications of fibrous dysplasia are visual impairment and hearing loss. Proptosis is the most common sign, with downward displacement of the eyeball and loss of visual acuity close at its heels. Other signs include sinus collapse, nasal obstruction, extraocular muscle palsies, trigeminal neuralgia, anomia and epiphora.
- Visual impairment and hearing loss constitute the most common neurologic complications of fibrous dysplasia. About 0.5 - 1% of all cases of fibrous dysplasia go on to turn malignant, the most common malignancy being osteogenic sarcoma, followed by fibrosarcoma, chondrosarcoma, and malignant fibrous histiocytoma.
- One should always check for café-au-lait spots in patients with fibrous dysplasia as it might be part of McCune-Albright syndrome.
Diagnosis of Fibrous Dysplasia
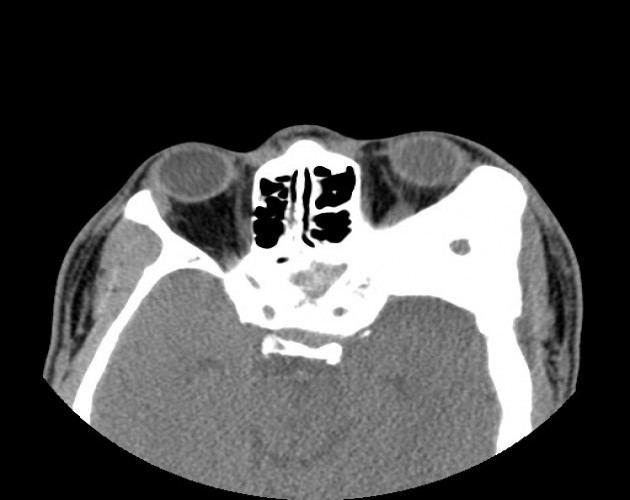
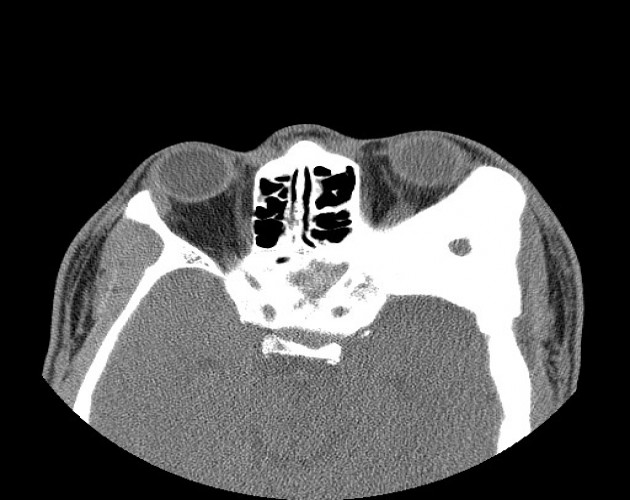
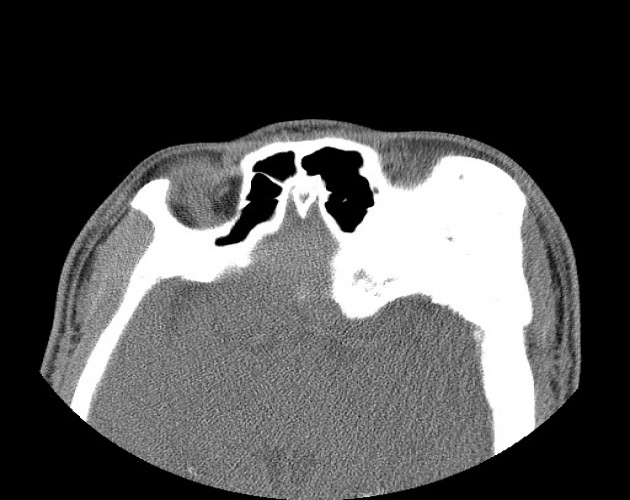
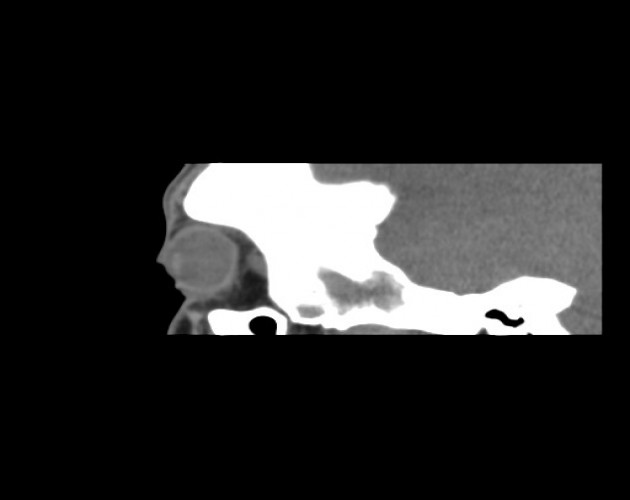
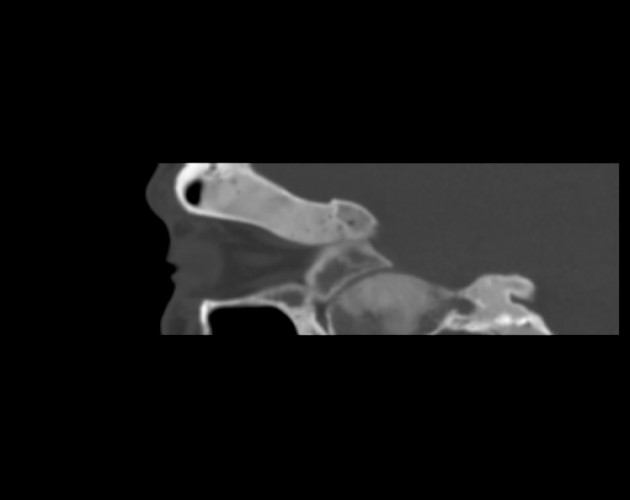
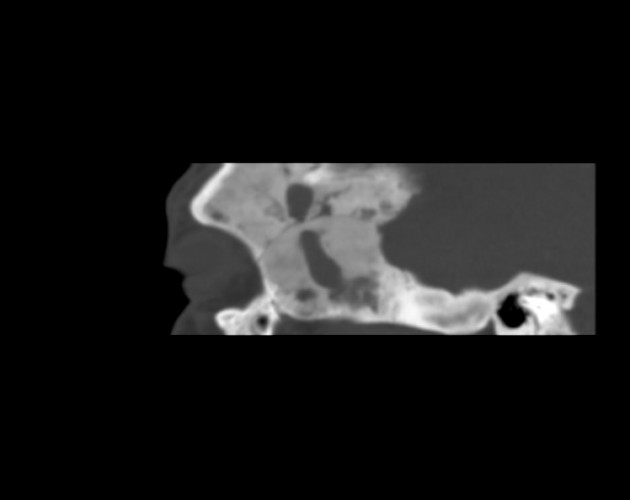
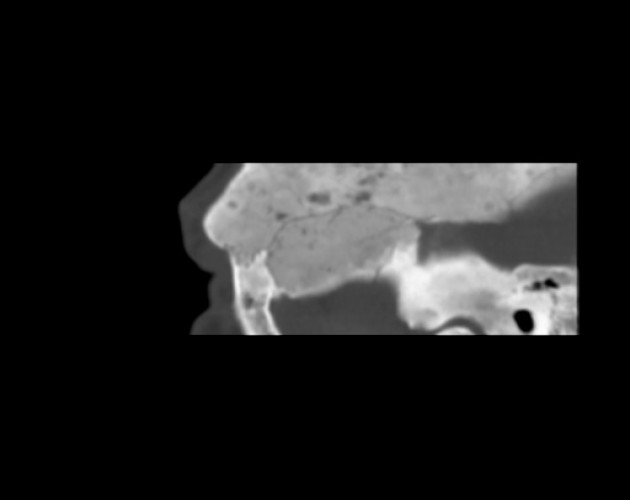
- The initial test recommended in a suspected case fibrous dysplasia is X-ray which shows characteristic mottling and sclerotic changes with a “ground-glass” appearance. Computed Tomography clearly shows cystic and sclerotic lesions with smooth cortical margins and no soft tissue involvement. MRI shows low to isointense lesions on T1 and T2-weighted images, and demonstrates moderate enhancement with gadolinium.
- About one-third of patients with fibrous dysplasia present with elevated levels of serum alkaline phosphatase. Fibrous dysplasia should be differentiated from meningioma, Paget’s disease or other osteodystrophies of the skull base, eosinophilic granuloma, Hand-Schuller-Christian disease, and low-grade central osteosarcoma which present in a similar fashion.
Treatment of Fibrous Dysplasia
- Fibrous dysplasia has a good prognosis with very little chance of cancer development. The disease is often self-limiting, and usually stabilizes with bone maturation. Treatment is guided by disease severity and progression and might involve simple observation or surgical intervention.
- Patients with mild disease are managed with diet and exercise targeted to maintain bone density and regular follow-up with imaging studies. Watch out also for visual impairment due to canal compression.
- Bisphosphonates are often prescribed to prevent bone resorption, with improvement in pain, biochemical markers, and resolution of radiographic lesions with regular use.
- Surgical intervention is the mainstay of treatment for symptomatic fibrous dysplasia. It is done in case of severe disfigurement, pathologic fractures, and other complications such as visual impairment. Therapeutic optic nerve decompression is done to preserve visual function. Recurrence after radical surgical resection is rare, but disease progression remains unabated with conservative surgery.
Procedures
- Anophthalmos
- Blepharoplasty
- Blepharospasm
- Brow Lift
- Congenital
- Dry Eye
- Eyelid Laxity
- Face
- Infections
- Inflammation
- Lacrimal System
- Lagophthalmos
- Latisse
- Locate an MD
- Orbital Tumors
- Ptosis
- Skin Rejuvenation
- Skin Tumors
- Symblepharon
- Thyroid Eye Disease
- Trauma

